Many people suffer from ear problems during and after diving. Technical rebreather diver and underwater photographer Dr Michael Rothschild is an ear, nose and throat specialist in New York City. In this series, he walks us through some of the common causes of dive-related ear problems, and how to treat and prevent them.

Contributed by
I am an avid scuba diver and an ear, nose and throat specialist, which means that I end up answering a lot of questions about this topic! The majority of medical problems encountered by divers involves the ears. While they are rarely as serious as decompression sickness or other life-threatening conditions, they are incredibly common and can ruin a dive trip.
In the last installment of this series, I discussed conditions affecting the outer ear. We now turn to the problems of the middle ear, and their prevention and management.
The middle ear
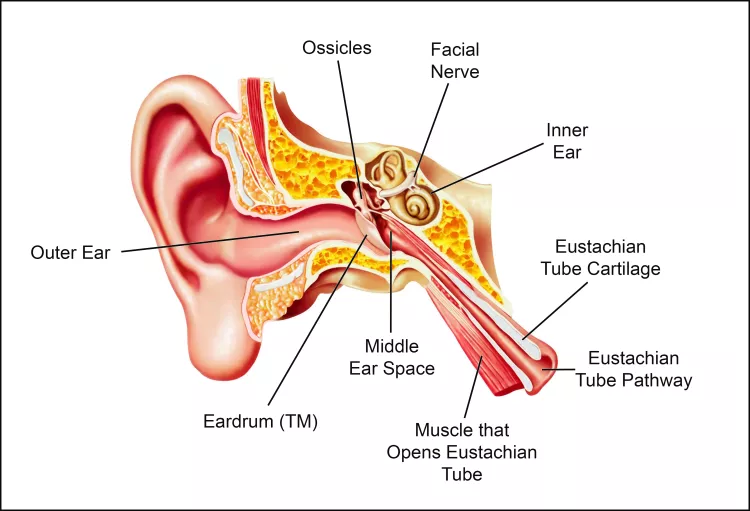
The middle ear is the space behind the eardrum (also known as the tympanic membrane, or TM). It is lined with mucosa, which is the same sort of “skin” that lines the mouth and nose. It also contains the three bones of hearing, known as “ossicles,” which carry sound vibrations from the eardrum to the inner ear, where they are converted into electrical impulses that are sent to the brain (see illustration).
The middle ear is basically an extension of the upper airway (the nose and throat), and it is connected to the back of the nose by a pathway called the Eustachian tube (ET). The walls of this pathway are supported by cartilage, which springs back to the normally closed position after being opened. This opening can be active—for example, by the muscle action of ear-clearing maneuvers on descent. It can also be passive, as gas flows from the middle ear back into the airway during ascent.
Diving injuries to the middle ear are the result of barotrauma, which is damage caused by gas pressure changes. As every certified diver knows, diving requires equalization of the pressure outside of the body with that inside, otherwise a gradient builds up. In the ear, this refers to a difference in pressure between the middle ear and the outer ear, across the TM. This can cause pain and eventually damage. Since fluid is essentially non-compressible, there are only significant pressure gradients in the air-filled spaces of the body.
Most of the air in the body is in the airways—the lungs, the windpipe, the larynx (voice box), the throat, mouth and nose. All of these spaces are connected by wide passages, so pressure changes occur everywhere at once in the airway, as a regulator delivers gas at ambient pressure (proportional to depth). It is possible to get a pressure gradient in the lungs—usually due to internal blockages of the air passages or by closing the larynx and holding the breath while ascending. While this is potentially serious, it is also quite rare.
There is also a small amount of air in other spaces in the body—the middle ear, the nasal sinuses, and sometimes the teeth (underneath dental work). These spaces are connected to the airways as well, but by small passages that may be blocked. Therefore, it is possible to build up a big pressure gradient in these spaces during descent and ascent, if a diver is not careful to equalize fully or if there are anatomical issues preventing equalization.
Equalization techniques and problems
To equalize the ears, the ET must be opened in the presence of a pressure gradient. This can be done by a number of maneuvers taught in basic open water scuba instruction. Pinching the nose and blowing (Valsalva maneuver) or pinching and swallowing (Toynbee maneuver) are common methods for equalization, but many divers learn to open the ET by other approaches, such as moving the jaw, tensing the roof of the mouth, etc.

A failure to equalize on descent can result in a “block”—a situation when the pressure gradient itself makes it harder for the ET to open, which results in a further gradient if descent is continued, leading to a vicious cycle and potential injury. The solution here is to stop the descent (or ascend a bit if necessary) until equalization is possible. If equalization is not possible, the dive must be aborted.
A less common situation may happen on ascent. With a poorly functioning ET, the change in middle ear gas pressure lags the change in ambient pressure. That means that during ascent there is higher pressure in the middle ear than in the airway (the reverse of what happens on descent). Because of this, the pressure gradient may be able to overcome ET dysfunction (ETD) as the air “forces” its way out. Think of how it is easier to squeeze toothpaste out of a tube than to put it back in. If this does not happen, a “reverse block” occurs, with worsening pain on ascent. Of course, even in the unusual case that a diver cannot equalize on the way up, eventually they must surface, no matter what the consequences for the ear.
Barotrauma
A prolonged or significant middle ear pressure gradient can result in barotrauma, also known as an ear “squeeze.” One common and sudden type of barotrauma is a perforated eardrum. The eardrum acts like the burst disk in the scuba tank—it is the weakest wall of the middle ear, and gives way when subjected to enough of a pressure gradient.
If the eardrum does not perforate, fluid with or without blood can accumulate in the middle ear space. Unlike the middle ear infections that young children get, this fluid is clean with no bacteria. Clear fluid is called an “effusion,” and a bloody effusion is called a “hemotympanum.” The effusion is actually the result of fluid in the bloodstream (plasma) filtering into the middle ear due to the pressure gradient. In very rare cases, middle ear barotrauma can cause weakness of the face, since the facial nerve controlling the muscles runs through the middle ear.
Fluid in the middle ear causes a hearing loss by impeding the normal transmission of sound vibrations through the middle ear from the eardrum to the inner ear. It is a “conductive” hearing loss—the problem is that the mechanism that conducts sound is not working well. The other type of hearing loss is a “sensorineural” hearing loss, which implies a problem with the sensory organ (the cochlea) or the nerves to the brain. Conductive hearing losses are usually temporary, as compared to the almost always permanent sensorineural loss, which we will discuss in the next section.
Some people have more trouble with this than others, due to inherent ETD. Many divers always need a long time to descend and ascend since their ETs do not work very well at baseline. Other people may have no problem equalizing in general but find it more difficult when a cold or other infection causes congestion of the lining of the ET. This is often oversimplified as the ET being “small” or “narrow”—the true problem is usually more of a technique issue than a structural one.
Another common misconception is that fixing nasal obstruction—for example by straightening a deviated nasal septum—will help the function of the ET. While there is some overlap between nasal blockage due to an upper airway infection and ET function as mentioned above, most of the areas of the nose that require treatment to improve breathing are nowhere near the ET opening.
Treatment

An eardrum perforation related to barotrauma (without a history of ear disease) usually heals by itself over weeks to months, but no diving is allowed until the eardrum is once again intact. In some cases, surgery will be needed to seal the hole in the drum. Middle ear effusion typically resolves over time, and can be helped to resolve by the same sort of ET opening maneuvers described above. Oral antibiotics are almost never needed.
Many divers swear by the use of decongestants and/or nasal steroid sprays to treat this problem or prevent its development. While these drugs can help prevent barotrauma of the nasal sinuses, there is not much data to suggest that they help middle ear disease any more than time and the ET maneuvers alone. Eardrops have no effect on the middle ear with an intact eardrum—while they can help with outer ear problems, they have no role in the treatment of barotrauma.
Oral steroids can help improve ET function in the days and weeks following a dive injury, draining an effusion, but these drugs have side effects and are not always necessary in this situation. Motrin and other non-steroidal anti-inflammatory drugs may help with the pain but have little effect on ET function. In some cases (when no more diving is planned in the near future), an ENT doctor can make a small hole in the eardrum to drain the effusion if it is causing severe symptoms, such as a hearing loss, or an uncomfortable blocked sensation in the ear.
There is not a lot that can be done directly to treat the underlying ETD. In young children, small tubes can be placed through the eardrum to temporarily ventilate the ears while awaiting for the ETD to resolve with growth. This is rarely necessary in older patients, although there is a new procedure (balloon dilation of the ET) that may be helpful in selected cases. There has not been a lot of experience using this in scuba divers, but early results seem promising.
For the vast majority of divers who have problems equalizing, the issue is technique and not anatomy. They may eventually address the problem by finding a maneuver that works to allow them to equalize. If the ETD is caused by a temporary problem (like a cold or other infection), then ear ventilation usually returns to baseline when the airway congestion resolves.
Conclusion
Most ear pain or hearing loss after diving goes away by itself in a short time. However, without an examination, a diver may not be able to tell whether the problem is in the outer, middle ear or inner ear, and treatment depends on accurate diagnosis. Thorough evaluation of persistent ear problems should be done by a doctor with the tools and experience necessary to distinguish these types of ear disease.
Next time, Dr Rothschild will discuss diving-related problems of the inner ear and how to manage them. See Part 3. Missed Part 1? Go to the article here. For more information, please visit: dive.rothschilddesign.com.





")