Many people suffer from ear problems during and after diving. Technical rebreather diver and underwater photographer Dr Michael Rothschild is an ear, nose and throat specialist in New York City. In this series, he walks us through some of the common causes of dive-related ear problems, and how to treat and prevent them.
")
Contributed by
I am an avid scuba diver and an ear, nose and throat specialist, which means that I end up answering a LOT of questions about this topic! The majority of medical problems encountered by divers involve the ears. While they are rarely as serious as other life-threatening conditions, they are common and can ruin a dive trip.
In the last installment of this series (in issue 115), I discussed conditions affecting the middle ear. We now turn to the problems of the inner ear, and their prevention and management.
The inner ear
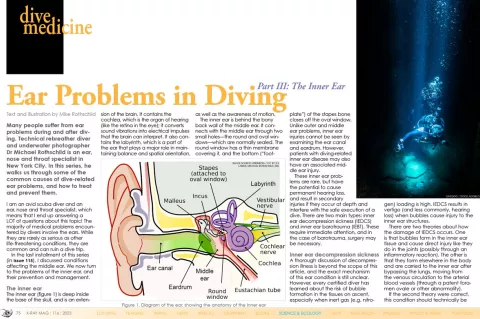
The inner ear (figure 1) is deep inside the base of the skull, and is an extension of the brain. It contains the cochlea, which is the organ of hearing (like the retina in the eye); it converts sound vibrations into electrical impulses that the brain can interpret. It also contains the labyrinth, which is a part of the ear that plays a major role in maintaining balance and spatial orientation, as well as the awareness of motion.
The inner ear is behind the bony back wall of the middle ear. It connects with the middle ear through two small holes—the round and oval windows—which are normally sealed. The round window has a thin membrane covering it, and the bottom (“footplate”) of the stapes bone closes off the oval window. Unlike outer and middle ear problems, inner ear injuries cannot be seen by examining the ear canal and eardrum. However, patients with diving-related inner ear disease may also have an associated middle ear injury.
These inner ear problems are rare, but have the potential to cause permanent hearing loss, and result in secondary injuries if they occur at depth and interfere with the safe execution of a dive. There are two main types: inner ear decompression sickness (IEDCS) and inner ear barotrauma (IEBT). These require immediate attention, and in the case of barotrauma, surgery may be necessary.
Inner ear decompression sickness
A thorough discussion of decompression illness is beyond the scope of this article, and the exact mechanism of this ear condition is still unclear. However, every certified diver has learned about the risk of bubble formation in the tissues on ascent, especially when inert gas (e.g. nitrogen) loading is high. IEDCS results in vertigo (and less commonly, hearing loss) when bubbles cause injury to the inner ear structures.
There are two theories about how the damage of IEDCS occurs. One is that bubbles form in the inner ear tissue and cause direct injury like they do in the joints (possibly through an inflammatory reaction). The other is that they form elsewhere in the body and are carried to the inner ear after bypassing the lungs, moving from the venous circulation to the arterial blood vessels (through a patent foramen ovale or other abnormality).
If the second theory were correct, this condition should technically be called decompression illness, since DCI includes both DCS and arterial gas embolism. However, the term IEDCS is standard usage.
Inner ear barotrauma
IEBT can happen in a number of ways, involving a sudden pressure change in the inner ear fluid (known as perilymph). A sharp increase in middle ear pressure happens with a rapid descent, especially with poor equalization. This can also happen with an overly forceful Valsalva maneuver, especially if the ET opens suddenly. This can cause the stapes (the bone between the middle and inner ear spaces) to be pushed into the oval window, resulting in a spike in perilymph pressure, potentially breaking the seal at the round window.
Alternately, Valsalva with a blocked ET can result in another type of rapid pressure gradient across the round window. Cerebrospinal fluid surrounds the brain, and increased CSF pressure from straining can be transmitted to the inner ear through a structure known as the cochlear aqueduct. The risk of injury is high if the ET is blocked and equalization is not adequate, worsening the gradient.
This sort of trauma can result in a “perilymph fistula” (PLF). Such a fistula causes leakage of inner ear fluid into the middle ear, potentially causing a progressive and often permanent hearing loss, as well as (less commonly) vertigo and nausea.
One other rare condition that can result in inner ear problems with diving is superior canal dehiscence, in which the bony covering of the inner ear is thin or missing. This can cause pressure changes to be transmitted directly to the balance organ of the inner ear.
Diagnosis of IEDCS and IEBT
Diagnosis of inner ear problems can be difficult, as the eardrum is usually normal on exam. Treatment for IEDCS and IEBT is very different, and recompression of a patient with IEBT can actually make the ear injury worse. Some authors have suggested that if the diagnosis is uncertain, holes should be made in the eardrums (myringotomy) before entering the chamber to prevent this complication. In actual practice, this is rarely necessary as the two conditions have different presenting features.
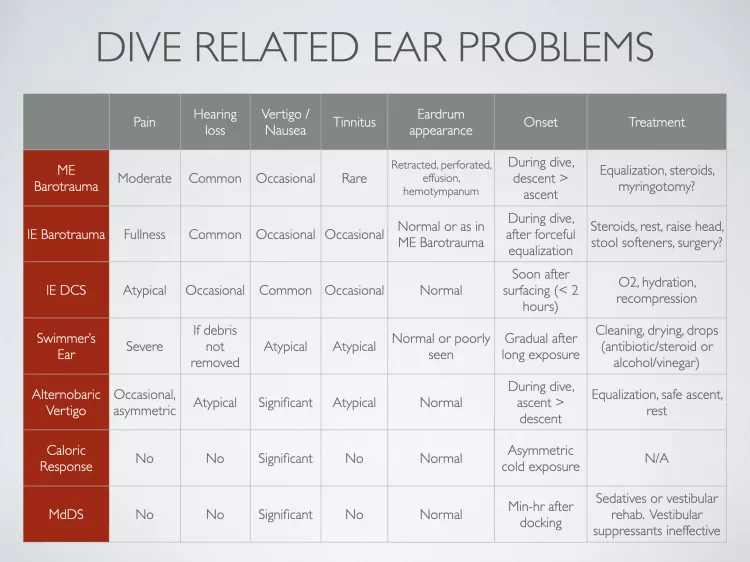
IEDCS may be suggested by the dive profile—excessive nitrogen loading, rapid or multiple ascents, aggressive decompression plans or skipped decompression stops. Also, there is usually a short symptom-free interval after surfacing, with the vertigo generally starting within two hours. Symptoms of IEBT, on the other hand, usually develop during the dive, often following a forceful equalization. In both conditions there may be nystagmus—rapid movements of the eye away from the injured inner ear. While vertigo is more common with IEDCS and hearing loss with IEBT, either of these can be present. See Table 1 for a summary of the different presentations of these two conditions, as well as other ear problems encountered by divers.
Prior to decompression, all patients with any sort of suspected decompression illness should be treated with 100% oxygen and hydration (if conscious and able to drink). Even if the diagnosis is actually IEBT, there is no harm of doing this, so this initial treatment should not be delayed because of any uncertainty.
A formal hearing test can distinguish between the conductive hearing loss seen in middle ear disease, and the sensorineural hearing loss of inner ear injury, and therefore should be a part of the evaluation of any diving-related ear problems. Other tests include an assessment of the function of the balance mechanism, which can be measured in a special lab. A CT scan is rarely helpful for the ear diagnosis itself, as an acquired PLF caused by barotrauma cannot be seen on an x-ray. However, a CT is often obtained prior to recompression to rule out other neurological conditions.
Treatment of IEBT
Initial treatment of IEBT involves limiting any further injury. Resting with the head elevated can help. Valsalva maneuvers should be avoided, as should any other type of straining (some doctors recommend the use of stool softeners). Heavy exertion, especially lifting heavy objects, can worsen IEBT. And diving should not be resumed until receiving clearance from an appropriate specialist.
When there is enough of a suspicion of a PLF, an operation may be recommended. This condition can only be definitively diagnosed by surgical exploration of the ear (you cannot see the inner ear fluid by looking in the ear canal). The procedure involves lifting up the eardrum to visualize the middle ear directly.
If what looks like inner ear fluid is seen leaking from the space around the round window (or anywhere else), fat grafts are used to seal the area. This leakage can be very subtle, as the volume of perilymph is small. However, early closure of a PLF can mean the difference between a recovery of hearing and a progression to complete deafness. Since the operation itself involves very little risk, it should be strongly considered in cases where PLF is a possibility.
Other causes of vertigo
Dizziness without the risk of permanent damage can be caused by other conditions that arise during diving. These have in common a lack of normal, symmetric inputs from the sensory organs of the ears to the brain. Either asymmetric signals from each side, or inconsistent information from the ears and the eyes will result in nausea, vomiting and/or vertigo—this is the brain’s response to such confusing inputs.
The balance organ of the inner ear (the semicircular canals) can be cooled by exposure to water in the ear canal, which causes the fluid inside the canals to move—this is a cold caloric response. If one ear is exposed to more cold water than the other (for example, from a poorly fitting hood or wax in one ear canal) the brain will get different signals from each ear. Similarly, if one ear equalizes before the other, there will be a pressure difference between the ears, with differential stimulation of the left and right inner ear sensory mechanisms. This is known as altenobaric vertigo.
Both of these conditions are generally temporary, and resolve as the temperature stabilizes and the flow stops, or as equalization is completed. However, it can be very disconcerting to have sudden dizziness during a dive. Awareness of this phenomenon and taking any steps necessary to address it (such as careful and thorough equalization) can prevent a spiral into panic and bad decisions.
Sea sickness
Another condition well known to boat divers is sea sickness. Here, the vertigo is caused by inconsistency between the inputs to the brain from the eyes and the ears.
If you are on a moving boat, your ears are telling your brain that you are moving up and down in space. But if your eyes are looking at any part of the boat, they will send the signal that you are standing still. This is why staring at the horizon helps—it coordinates the information received by the brain from the ears and the eyes.
A complete discussion of seasickness remedies would be too long for this article. But most people manage this condition with medications, best taken several hours before departure. First-generation over-the-counter antihistamines (like Benadryl or meclizine) are popular. Prescription scopolamine is also quite effective and is usually used as a patch that lets the drug pass through the skin. Other people have had success with acupressure wristbands or crystallized ginger.
Mal de Debarquement
Finally, there is the condition known as Mal de Debarquement (“the sickness of getting off a boat”). Some people are unsteady and have difficulty walking after reaching dry land. This is thought to be an issue with the brain’s adaptation to a new environment, and not an ear problem.
In such cases, inner ear testing is normal, but the symptoms may last for a long time (months). Treatment with vestibular suppressants (like Bonine or Dramamine) rarely works, but sedatives and specialized physical therapy (vestibular rehabilitation) may be helpful.
Conclusion
Most ear pain, dizziness or hearing loss after diving goes away by itself in a short time. However, without an examination, a diver may not be able to tell whether the problem is in the outer, middle ear or inner ear, and treatment depends on accurate diagnosis. Thorough evaluation of persistent ear problems should be done by a doctor with the tools and experience necessary to distinguish these conditions.
Read Part 1 on the outer ear and Part 2 on the middle ear. For more information, visit: dive.rothschilddesign.com.






")